
This post is intended as a round-up of available information on the current Ebola outbreak from various sources around the web. Corbett Report members are encouraged to debate and discuss the situation in the commments thread below, ask questions, suggest links, and otherwise contribute to this investigation. The comments will be used to piece together an upcoming episode of The Corbett Report Podcast on this subject [UPDATE: The podcast is now available for downloadhere]. [Not a Corbett Report member? Sign up today.]
Overview: Official information on Ebola virus
 Ebola haemorrhagic fever is the human disease caused by the Ebola virus. According to the World Health Organization (WHO), the disease has a fatality rate of up to 90% and is “one of the world’s most virulent diseases.” The disease first appeared in 1976 in two simultaneous outbreaks, one in the Congo (near the Ebola river) and the other in a remote area of Sudan. It transfers through close contact with blood of an infected animal (including chimpanzees, gorillas, fruit bats, monkeys, forest antelope and porcupines) and spreads human-to-human through direct contact with infected blood or other bodily fluids, or through contact between broken skin or mucous membranes of a healthy person and the contaminated possessions (blankets, bedclothes, needles) of an infected person.
Ebola haemorrhagic fever is the human disease caused by the Ebola virus. According to the World Health Organization (WHO), the disease has a fatality rate of up to 90% and is “one of the world’s most virulent diseases.” The disease first appeared in 1976 in two simultaneous outbreaks, one in the Congo (near the Ebola river) and the other in a remote area of Sudan. It transfers through close contact with blood of an infected animal (including chimpanzees, gorillas, fruit bats, monkeys, forest antelope and porcupines) and spreads human-to-human through direct contact with infected blood or other bodily fluids, or through contact between broken skin or mucous membranes of a healthy person and the contaminated possessions (blankets, bedclothes, needles) of an infected person.
Symptoms include “sudden onset of fever, intense weakness, muscle pain, headache and sore throat” followed by “vomiting, diarrhoea, rash, impaired kidney and liver function, and in some cases, both internal and external bleeding.”
There is currently no licensed or authorized treatment or vaccine for Ebola virus. Serum containing antibodies from previously infected survivors of Ebola disease was used to successfully treat seven out of eight patients in the 1995 Congo outbreak (although those results have been disputedrepeatedly), and other experimental treatments are currently being developed including monoclonal antibodies and prototype vaccines. Controversy has arisen in the current outbreak over the unauthorized use of an experimental treament (“Zmapp“) to treat two cases in the US (see below).
Timeline of the 2014 outbreak
On March 22 2014, an epidemic emergency is declared after an outbreak of Ebola haemorrhagic fever in southern Guinea. That day, Médecins Sans Frontières announces they have already deployed 24 nurses, doctors, logisticians and hygiene and sanitation experts to the country with 33 tons of supplies leaving France and Belgium on the way.
 By March 25th, the BBC reports 62 confirmed deaths from the disease, including five people in Liberia who died “after crossing from southern Guinea for treatment.” As the BBC report notes, “It is the first time Ebola has struck Guinea, with recent outbreaks thousands of miles away, in Uganda and the Democratic Republic of Congo.”
By March 25th, the BBC reports 62 confirmed deaths from the disease, including five people in Liberia who died “after crossing from southern Guinea for treatment.” As the BBC report notes, “It is the first time Ebola has struck Guinea, with recent outbreaks thousands of miles away, in Uganda and the Democratic Republic of Congo.”
On March 31st, Ebola is confirmed to have spread to Liberia where two sisters (one of whom has just returned from Guinea) are found to be carrying the disease. The death toll rises to 78 people.
In early April West Africa begins mobilizing to combat the spread of the disease, including sending health teams to border territories.
By May 27th the death toll rises to 187 and the virus is confirmed to have spread to Sierra Leone.
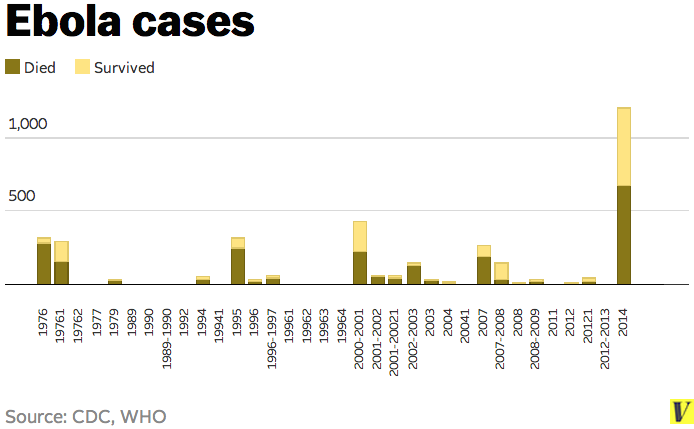
By mid-June, WHO data shows 333 total deaths, making this the deadliest outbreak in recorded history. The previous most deadly outbreak was the 1976 outbreak in Congo, with 280 reported deaths.
On July 3rd and 4th the WHO convenes a two-day Emergency Ministerial meeting on Ebola Virus Disease in Ghana where West African countries and various international organizations agree to adopt a strategy of “cross-border collaboration” for combating the outbreak. They also decide that the “WHO will establish a Sub-Regional Control Center in Guinea to act as a coordinating platform to consolidate technical support to West African countries by all major partners; and assist in resource mobilization” and that the WHO will be a lead organization in coordinating action on the issue.
The agreement includes resolutions to:
- Convene national inter-sectoral meetings involving key government ministries, national technical committees and other stakeholders to map out a plan for immediate implementation of the strategy.
- Mobilise community, religious, political leaders to improve awareness, and the understanding of the disease
- Strengthen surveillance, case finding reporting and contact tracing
- Deploy additional national human resources with the relevant qualifications to key hot spots.
- Identify and commit additional domestic financial resources
- Organise cross-border consultations to facilitate exchange of information
- Work and share experiences with countries that have previously managed Ebola outbreaks in the spirit of south-south cooperation
They also decide that the “WHO will establish a Sub-Regional Control Center in Guinea to act as a coordinating platform to consolidate technical support to West African countries by all major partners; and assist in resource mobilization.”
On July 25th the WHO confirms a probable case of Ebola in Nigeria, although an undated post on the Nigerian Federal Ministry of Health website claims to “debunk” Ebola in Nigeria, claiming that it is in fact Dengue Fever.
 On July 30th, Germany agrees to a WHO request to accept two Ebola infected patients for treatment at the university clinic in Hamburg-Eppendorf. According to Deutsche Welle: “The university clinic has made six beds available in a segregated part of the facility. In this isolation unit, no liquids, gases or particles in the air can reach the outside world. Access is only possible through three airlocks. In the first, the air pressure is slightly reduced; in the second and the third even more so. That’s to ensure clean air from outside is able to come in, but contaminated air from inside is not able to go out. Up until now, the unit has only been used for training.”
On July 30th, Germany agrees to a WHO request to accept two Ebola infected patients for treatment at the university clinic in Hamburg-Eppendorf. According to Deutsche Welle: “The university clinic has made six beds available in a segregated part of the facility. In this isolation unit, no liquids, gases or particles in the air can reach the outside world. Access is only possible through three airlocks. In the first, the air pressure is slightly reduced; in the second and the third even more so. That’s to ensure clean air from outside is able to come in, but contaminated air from inside is not able to go out. Up until now, the unit has only been used for training.”
On August 2nd, an infected American aid worker traveled from Liberia to the United States to receive treatment at Emory University Hospital in Atlanta. According to Reuters: “The facility at Emory, set up with the U.S. Centers for Disease Control and Prevention, is one of only four in the country with the facilities to deal with such cases.” A second American aid worker, also infected in Liberia, arrived at the same facility two days later.
As of August 6th, the disease is confirmed to be spreading in Guinea, Sierra Leone, Liberia and Nigeria. Suspected cases are currently being tested in Lagos, the Philippines, and Saudi Arabia. The total number of confirmed cases stands at 1,711 with 932 deaths. An emergency meeting of “global health experts” has just been convened by the WHO in Geneva to address the situation.UPDATE: On August 8th, the WHO declared the current Ebola outbreak a “Public Health Emergency of International Concern” This is an instrument under the International Health Regulations, a legally-binding international agreement on disease prevention and control. The declaration allows for potential international coordination of the crisis and grants the WHO powers to obtain and share information about the crisis anywhere within the IHR territories with or without the consent of the individual governments involved. According to Stephen Morrison, the director of the Global Health Policy Center at the Center for Strategic and International Studies, this potentially allows for “boots-on-the-ground” intervention by the US military or other NATO member countries to operate in these environments in terms of ground transport, supply chain, and distribution of commodities. This is only the third time a PHEIC has been declared, the first being the 2009 swine flu outbreak and the second a declaration related to polio earlier this year.
Controversies, Contradictions and Conspiracies
Despite repeated denials and downplaying of the possibility by health authorities, there is growing evidence that this strain of Ebola may be airborne (transmissible from human to human through the air, not direct contact). A 2012 study examining “Transmission of Ebola virus from pigs to non-human primates” concluded: “Our findings support the hypothesis that airborne transmission may contribute to ZEBOV spread, specifically from pigs to primates, and may need to be considered in assessing transmission from animals to humans in general.” Despite the fact that even the official CDC guidelines for how airlines should handle the Ebola crisis contains the concern tha the virus may be airborne, a concerted effort is being made online to ridicule those hypothesizing that the current Ebola outbreak represents an airborne strain of the virus:
According to Bloomberg: “Despite the deadly nature of the disease, the relative rarity of outbreaks and their confinement to primarily rural areas of poor African nations make Ebola an unattractive target for big drugmakers.” An American or German outbreak, would, of course, change that calculus, and just last month a potential treatment for the disease was put on hold by the FDA due to safety concerns. Now, controversy is arising after experimental medicine was given to the two stricken American aid workers without FDA approval. The BBC describes the medicine as a “ZMapp drug, which has only been tested on monkeys.” For many, the idea that the WHO is heavily involved in a pandemic emergency in which drug companies are looking to circumvent traditional approval processes raises eerie parallels with the 2009 swine flu scare, which followed this pattern almost exactly, and was later ruled by both the British Medical Journal and the Council of Europe to have been a sham pandemic declared by a Big Pharma-connected WHO panel on behalf of the vaccine manufacturers themselves.
Others point to the possibility that this Ebola has been weaponized, or is part of a plannedbioterror release. These reports focus on Dr. Charles Arntzen, a researcher at the University of Arizona who helped develop the experimental Ebola treatment given to the two American aid workers. In 2012, Dr. Arntzen joked about using genetic modification to create a “better virus” tocull 25% of the human population:
This is in line with similar statements by fellow biologists, including Dr. Eric Pianka at the University of Texas at Austin, who eyewitnesses claim used his acceptance speech for the 2006 Distinguished Texas Scientist Award from the Texas Academy of Science to muse on “the elimination of 90 percent of the human population” through an airborne disease like the Ebola virus.
Some have pointed to the long, documented history of government research into biological weapons and intentional government releases of biological agents on their own citizens in the past as a sign that the current outbreak could be some form of intentional bioweapon release by a government agency or rogue actor.
Yet others argue whether the current outbreak is being deliberately downplayed to hide the severity of what is happening or deliberately overhyped to panic the public and make them acquiesce to medical martial law or other dramatic maneuvers. Some even question whether or not the entire pandemic is a hoax.
By James Corbett, corbettreport.com